


A question for your friends:
If you contradict your government’s policy position on social media, should you be silently silenced? Especially when it concerns health 'facts'?

3200 words.
Our governments certainly want to prevent us from being misinformed and it seems that 2022-2023 is the time to do it. But what are we being misinformed about? What are we not talking about, that perhaps we should? Bryce Edwards has aptly described the election campaign as hollow and empty. An election without inspiration.
I speculate that a major driver is the important issues are increasingly taboo. If they are discussed, it’s at such a shallow level that they’re either polarising or uncompelling. They involve themes that are distasteful to the ‘Bigs’ - Big Pharma, Food, Development, Banking, Media, Agribusiness, Tech. Oligopolistic mega-corporations that are predominantly offshore-owned. They involve shedding light on power relations between these chaps and executive government. Identifying the influence of the IMF and external global banks and our Reserve Bank and the executive government. They involve discussions on the role of the military, and the secrecy and power of the security state. Discussions on the unfortunate habit of transferring decision-making powers from the regions to Wellington. They involve, very simply, a failure to discuss the institutional drivers that drive democratic decline, chronic illness, debt, and pollution.
Therefore, we’re getting frustrated and we’re trusting less. But as Palmer and Butler have said
‘Trust is at the heart of any successful nation. Trust breeds legitimacy and legitimacy breeds loyalty.’
When trust declines, what is left? Censorship, coercion and control?
BULDING THE CENSORSHIP PLATFORM
I’ve been trolled, I’ve seen the squabbles online when people get frustrated and I’m aware of a tiny, tiny minority that would easily come under existing legislation. But what I’ve also seen is the squabbles resolve in different ways. People learn, people get hurt, and then they meet for a beer. Sometimes they don’t. We’re ‘oooman. That’s what we do. It’s necessary. Democracy is only safe when we can squabble.
I suspect that New Zealand’s Department of Internal Affairs (DIA) ‘Safer Online Services and Media Platforms’ consultation will ratchet up power for the behemoth DIA. The new system would retain powers of censorship for the most extreme types of content (called ‘objectionable’ material).

What I have seen for about five years now, are consultations where the public are invited to submit, to present to Select Committees etc, and where thousands and thousands of people do. But their words fall on dry earth. The bureaucratic box has been ticked.
I am concerned the DIA will largely ignore the public again. I say ‘again’ - see PSGR’s submission to the Digital Identity Services Trust Framework Bill. Who needs human rights anyway when big corporations are working closely with governments.
It is quite easy to change the definition of ‘objectionable material’ to include content that contradicts government policy. Could disinformation, false or misleading information, that is purposefully distributed - be categorised as objectionable material? When the ‘false or misleading’ content is content that contradicts a policy position?
All Cabinet has to do is include ‘disinformation posted during a state of emergency’, (which can be now announced after heavy rainfall or when an infectious disease is highly transmissible but doesn’t result in a high case fatality rate).
It’s not just New Zealand that is aiming to ‘protect’ us for our ‘safety’. The 2022-2023 flurry of legislation and policy resulted in South Africa’s’ Films and Publications Amendment (FPA) Act (March 2022); Europe’s’ Digital Services Act (Nov 2022); the UK’s Online Safety Bill (Sept 2023); and Canada’s ‘transparent and accountable regulatory framework for online safety’ (in play) show us the lock-step trajectory. Australia’s Social Media (Protecting Australians from Censorship) Bill 2022 appears to have lapsed. The US is more uncertain and seems to be countering the online safety-fest.
It’s certainly not ground-up governance.
The lock-step pattern, an increasingly powerful executive, and under-resourced MP’s suggest policy dev is top down.
How closely entangled is the New Zealand government with social media corporations? Agencies regularly engage with Facebook on operational issues, and Internal Affairs/Te Tari use the Meta / Facebook Reporting system to notify of objectionable content. We don’t know the extent to which the Department of Internal Affairs Digital Safety Group limits the reach of ‘certain users’. Can we query whether the Christchurch Call with Ardern in play, produces broader opportunities for censorship than perhaps the public imagine? It seems to me the government is happy to talk about the Christchurch Call, but not so keen to disclose the nature of relationships and the extent of suppression of accounts with/by Twitter.
Then there is the Harmful Digital Communications Act 2015, administered by the Ministry of Justice. Where ‘harm’ is defined as ‘serious emotional distress’. Then there is Principle 6…
Principle 6. A digital communication should not make a false allegation.
What happens if a false allegation (see S.6 & 22) is simply seen as someone contradicting the government’s policy position?
COVID-19 MEDICAL MISINFORMATION BY OMISSION
Netsafe’s How to Spot Fake News April 2021 article advised us that the most ‘accurate’ health information on COVID-19 came from the Ministry of Health, covid19.govt.nz or Hāpai Te Hauora websites. Was fake news, information that contradicted this ‘trusted source’?
Ministry of Health COVID-19 messages continue to decorate YouTube content. The extent of government-directed warnings plastered to information Kiwis posted during COVID-19 will remain unknown. What will also remain unknown is the extent of deplatforming and flat-out censoring, because individuals and organisations contradicted the government’s policy position from 2020 onwards.
If governments cannot protect speech and the sharing of information that contradicts or challenges government policy positions, freedom is lost.
Why? Perhaps it’s because governments fail to make a space for science and research that contradicts the vast amount of data and information produced by private industry, so officials will do what they’re told by the elites. There’s nowhere else to run.
Funding is selective. Expansion of budgets for pharmaceuticals isn’t a problem; but governments in parallel, ignore and fail to make a space for contradictory science, science that might upset a policy trajectory or challenge the claims of the pharmaceutical and biomedical industry. This funding is no go.
Misinformation is driven by governments when they prioritise pharmaceutical industry science and fail to conduct peer reviewed science that might contradict industry position. Medical doctors then trust the government’s position. We shouldn’t ignore corporate influence when it comes to protecting environmental and human health.
As COVID-19 demonstrated, official medical policy and information directed the public to expensive newly patented drugs, not well trodden, off-patent drugs. The richly funded networks directing policy to fund and prioritise mRNA injections over established drug pathways for respiratory viruses were extensive.
Conflicts of interest drive the capture of academic researchers and regulatory agencies. Medical misinformation is driven by governments when their legislation for approving drugs circles around industry data, even though illegal activity is relatively common. It’s driven when governments and pharmaceutical companies fund media.
Misinformation occurs when governments fail to consider the broader evidence in the literature, and only look at the results of randomised trials. Because when it comes to less toxic alternatives of nutrients and off-patent drugs with a strong safety profile, we can take into account case reports, case control studies and cohort studies. We can also look at the experiences of individual people. Because N=1.
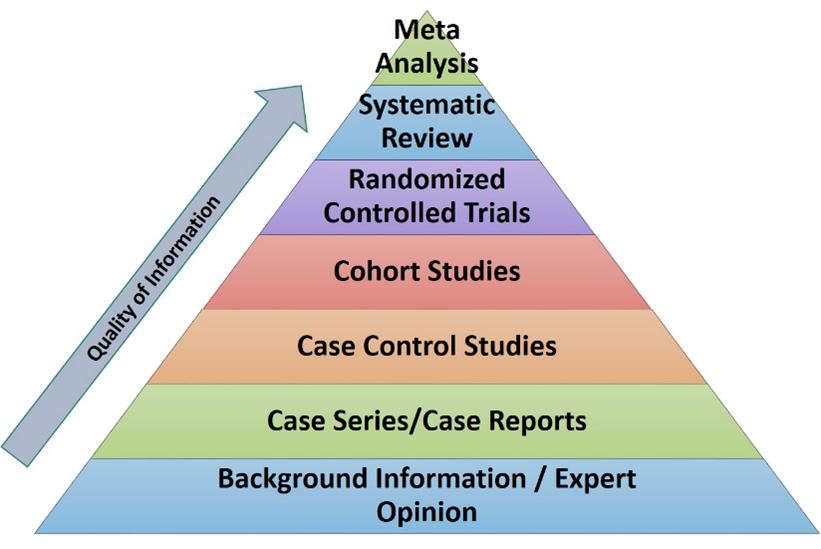
It often appears from government literature that the only way government can adopt a treatment is by waiting for the results of a randomised clinical trial (RCT)? If government doesn’t, they’re not scientific enough. But then perhaps, a few trials are required, especially if they’re underpowered (not enough people). Then you need to wait a few years for a meta-analysis. Then, perhaps you have to discount a few trials (like Cochrane did with vitamin D). Perhaps then.
But how risky is a brand-new drug; compared to an off-patent drug or vitamin with an extensive safety record, in the peer reviewed literature, or a dietary change?
Sir Austin Bradford Hill’s 1965 argument that could strengthen consideration around whether epidemiological associations might be considered causal can be adapted for modern use. While Bradford Hill was concerned with environmental chemicals, reviews could consider the role of nutrition.
MEDICAL TREATMENTS ARE NOT A PROXY FOR HEALTH
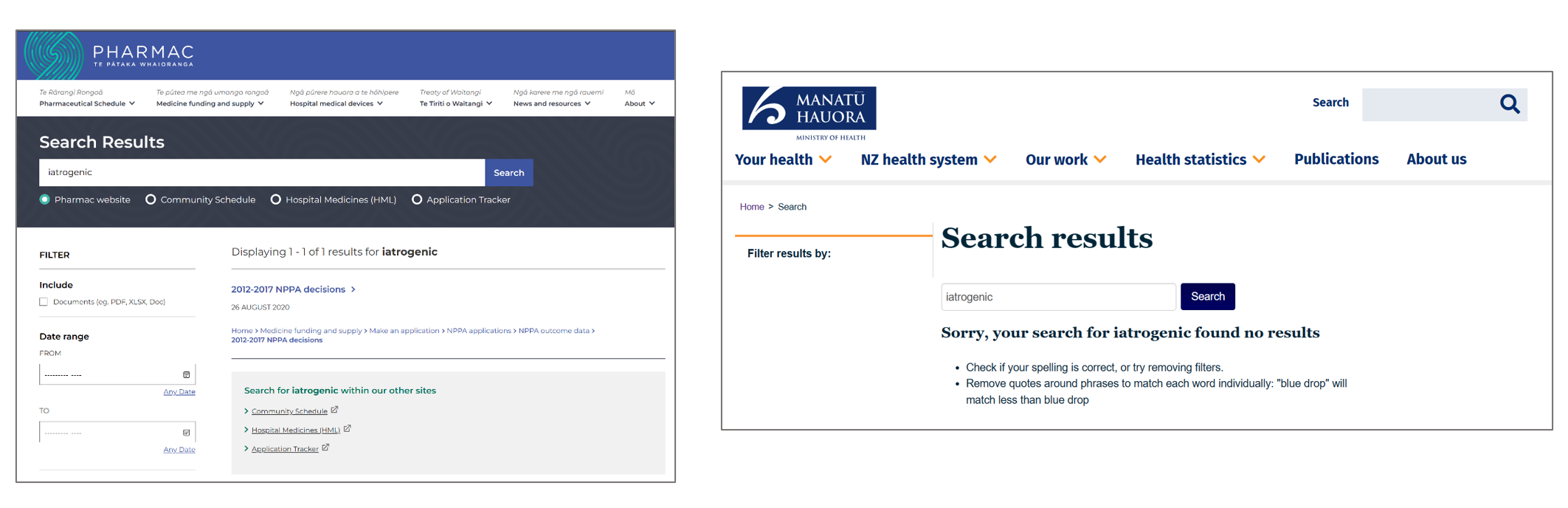
Yes, when making public-health recommendations at the population level, caution is warranted. However, at the public health level, I neither see disclosures nor education to inform the public on the extent to which iatrogenic harm drives hospitalisation and death. In the USA medical treatments are the third leading cause of death. Doctors spend a lot of time navigating medical risk, and I suspect, pharmacists spend even more time avoiding Bad Stuff Happening. Sorry, no long-term funding for this in New Zealand so only spotty information on Google Scholar.
When governments fail to acknowledge the extent to which iatrogenic risk is a problem, they also drive medical misinformation.
When governments ignore the risk of new classes of drugs, they also drive …
When were the public privy to discussion in the Therapeutic Products Bill on the instability and risks of biologics? The Therapeutic Products Bill did a nice job of emphasising how risky nutritional therapeutics are, while (old Medicines Act) quietly inserting biologic drugs (new Therapeutic Products Act) in the legislation. This was in effect a massive deregulatory effort, it prevented civil society from acting. From requiring that the Minister in charge put special regulatory requirements in place for biologics. The shiny thing is over here, not there! But well, Parliamentary debates and Select Committees really don’t want to talk about pesky issues such as that.
Will we be censored, deplatformed, shadow-banned or deboosted following Twitter’s ‘freedom of speech not freedom of reach’ policy, – when the next biologic drug is mandated, no matter how weak the legislation and how narrowly formed the policy?
LEGAL OBLIGATIONS OF THE MINISTRY OF HEALTH
All Ministry of Health (and other) officials acting under the Health Act are required to improve, promote, and protect public health. Te Whatu Ora, Health New Zealand is also established to protect, promote, and improve the health of all New Zealanders – in addition, officials are required to promote health and prevent, reduce, and delay ill-health.
When nutrition and diet cannot be discussed nor the scientific literature drawn upon with respect to the data in the peer reviewed literature, officials charged with administering these Acts fail in their duty.
When the government fails to undertake research and funding to kind a, well do this work, their duty, are online statements that contradict the government’s policy position, false allegations?
While drugs are touted, our agencies Te Whatu Ora, Ministry of Health consistently fail to promote diet and nutrition as a driver of risk from chronic and infectious disease. Te Whatu Ora is to all appearances, a vaccines promotion agency.

Even though the word ‘health’ is in the legislation their policies are much more likely to concern the deployment of medicine. We see this on the Ministry of Health website.
MINISTRY OF HEALTH MEDICINE
The Ministry of Health’s Strategic Intentions 2021 to 2025 white paper, focuses on medical treatment and mental health services, hospital care and behaviour modification. The High-level Indicators demonstrate the department prioritises injections, hospital admissions and access to medical treatment. Not reversal of reversable diseases.
Food policy, diet and nutrition are not mentioned.
The term ‘healthy’ is mentioned frequently in the Strategic Intentions document without any policy basis to demonstrate an attempt to reduce diet-related diseases.
‘The Ministry is committed to achieving pae ora - healthy futures.’ The Ministry is committed to ‘living longer and healthier lives.’
This is contradicted as lives are increasingly lost due to disability and disease. We are living more years suffering from sickness and/or disability. But
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.
Health is not a suppression of symptoms and ignorance of the drivers of metabolic disease. This policy fails Māori and non-Māori, because it presumes you can have many disease conditions and that is health and well-being. It’s bullshit. All policies lead to treatment and care for an increasingly sick population.
What the Ministry of Health consistently fail to do is emphasise the extent to which diet - ultraprocessed foods - drives the tsunami of chronic disease and mental illness. This is downplayed, ignored, sidelined.
EQUITY OF HEALTH - NOT EQUITY OF PRESCRIBING MEDICINE
Information is driven when governments fail to signal that a certain intervention is far less risky than existing drugs, and there is substantial literature supporting a non-pharmaceutical intervention.
But the structure and function of the Ministry of Health and the agencies that it administers and associates with, drive the status quo.
But MoH are not responsible for science production to understand the drivers of disease, and they take their lead on new medications from Pharmac. Pharmac’s legislation doesn’t require Pharmac to provide vitamins and minerals for the public. Pharmac of course, is required (Part 4)
‘to secure for eligible people in need of pharmaceuticals, the best health outcomes that are reasonably achievable from pharmaceutical treatment and from within the amount of funding provided.’
Pharmac are not going to review the dietary and nutritional literature. Pharmac might require rigorous vetting processes to approve a nutritional therapy (i.e. through a psychiatrist or oncologist instead of a G.P.) but that’s because they conventionally think like the pharmaceutical industry. It’s difficult to think of the bioavailability and long cultural use of a nutritional therapy. This leads to other gaps in knowledge when for example, funding for free testing for vitamin D is not available.
It’s not surprising that the Ministry of Health and Pharmac conflate the risk of dietary changes, or micronutrient therapies, with the same level of risk as pharmaceutical medication, as we saw in with the Therapeutic Products Bill consultation. The average official is ignorant by design.
Then, the private but powerful New Zealand Medical Council (NZMC) discourage doctors from prescribing nutrients. Medical doctors are trained in prescribing medicine, so very few try to challenge the NZMC’s position.
But then, as I’ve found, New Zealand government policy steers scientists and researchers away from looking at diet related reversal of disease. Doctors won’t be informed. There won’t be funding for major RCTs in New Zealand on dietary reversal of major conditions, this sort of research is not in scope for funding.
Structure and function. And it’s not as if the red-blue Ministers of Health have had any reason to change for nearly a hundred years.

THE EVIDENCE IS GROWING: MOH’S POLICIES ARE FLAWED
Here’s a charge: The Ministry of Health firstly, drives misinformation by failing to assess the substantially lower risk profile of nutritional therapies and dietary interventions; and secondly, fails to inform the public of the benefits of shifting from an ultraprocessed diet.
Diet changes have the potential to not only transform and ‘even’ reverse a startling range of chronic conditions, and are immunoprotective against respiratory viruses. We would think that the Ministry of Health (MoH) would take a deep dive into this.
But no.
You probably know about the strong association of diet in reversing the risk factors for heart disease and the increasing evidence for dietary changes in reversing diabetes. Then there’s macular degeneration, also associated with diabetes and diet. Alzheimer’s disease is increasingly referred to as type 3 diabetes, because the disease is associated with blood glucose levels and impaired insulin function.
It’s also likely that you don’t know the extent of important scientific research shedding light on how dietary changes, and micronutrient supplementation can ameliorate and even reverse mental illness/challenges including depression, anxiety, ADHD, autism and schizophrenia. Two great podcasts interviewing scientists can be found (1) YT here, Spotify here; and (2) YT here and Spotify here.
As I’ve said before, the government certainly doesn’t seem to know this.
Did you know that research into diet to reverse epilepsy is over one hundred years old, and that the epilepsy knowledge spurred cancer researchers to take a look at using the same protocols to reverse cancer? Seyfried’s book Cancer as a Metabolic Disease: On the Origin, Management, and Prevention of Cancer, is now a decade old, and rather than being debated by conventional oncologists, he’s just ignored. (Lisa Tamati isn’t ignoring Seyfried though!).
Current policy to address cancer is failing miserably.
Oh and don’t talk about major policy that could shed light on dental health and fermentable carbohydrates (sugars and starches) from processed food, because it’s all about the non-nutrient fluoride, not any real nutrients that promote strong teeth.
Informed consent is impossible in this environment. Young people are ushered onto drugs without being given the choice of a non-pharmaceutical intervention.
Why don’t our health authorities talk about how compelling the evidence is, and what might happen across a wide range of conditions?
Our under-resourced MPs don’t have a hope in hell. Governments understand there is an increase in productive years lost due to preventable disease; and that young people, are being ignored in health policy, and are consuming more medical drugs than previous generations.
The result is over-prescription (it’s not me saying it, it’s scientists and doctors) of in-patent statins, pandemic drugs (mandates for healthy people), drugs for mental health conditions, and cancer drugs (when earlier dietary intervention to could reduce risk from harm from oncology treatments).
There are other choices patients should have that are arguably more powerful, arguably less risky, and arguably that provide complex benefits than a course of drugs. Noting that multimorbidity (not single conditions), is the norm, and that the cost of treating patients with multiple health conditions is scalar.
This is why they say, well, there’s no evidence because we don’t have any RCTs to prove it. You’re damn right. Who wants to do a peer reviewed trial for an off-patent drug or nutritional therapy where you don’t own the I.P.? None of ‘em. We saw Merck shying away from clinical trials for their own product ivermectin during COVID-19.
THE MINISTRY OF HEALTH: DRIVING MISINFORMATION BY OMISSION
Since 1935, the only Ministers of Health have been Labour or National Ministers. Ministers from these two parties have held extraordinary power in the health medical system for nearly 90 years.
When all these pathways lead us away from dietary nutrition, is it disinformation, false or misleading information that is purposefully distributed? Is there a deliberate effort to ignore diet as a driver of disease?
Let’s go back to the start - that false allegation. What will the censors do in the next health emergency? We know all the work the government is not doing is omitting to do to protect health.
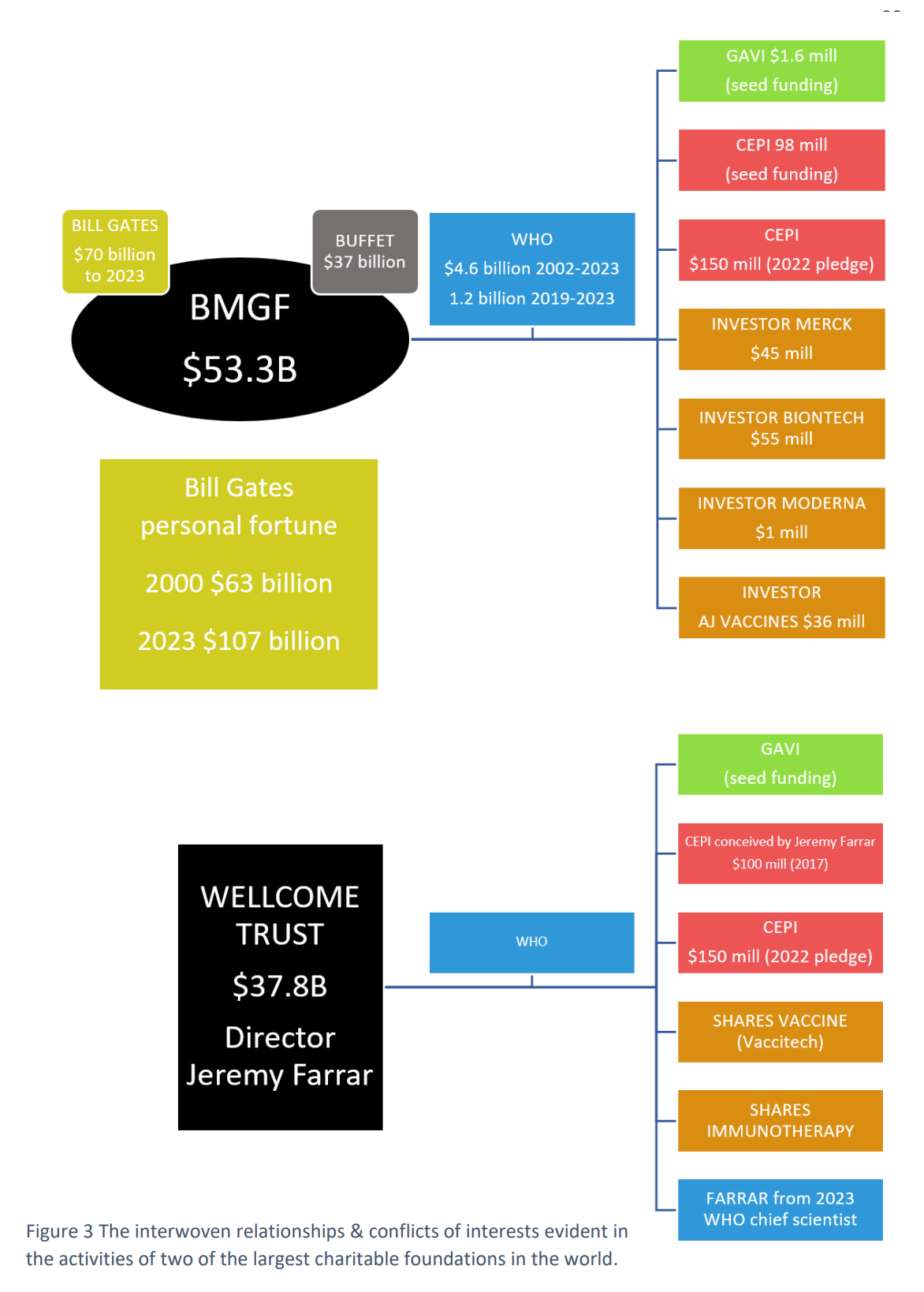
What if the false allegation (under the Harmful Digital Communications Act 2015) results from angry criticism of a World Health Organisation decision in the ‘next’ pandemic, if our MPs silently acquiesce to WHO control?
Government and social media censors won’t take into account the WHO’s institutional conflicts of interest, will they? WHO donations are mainly earmarked (specified). As David Bell states:
The WHO has become a conduit through which a funder can implement programs from which they stand to benefit.
Please keep talking. Please keep asking your mates what they think. Even if it is uncomfortable.
Channel your inner Socrates, curious not angry.
In the days leading up to election day, October 14, 2023, perhaps, take a gander at all the parties registered on the ballot, see who is active in your electorate, and look at their health policies. If your preferred party doesn’t talk about this stuff I’m raising here, after decades of the red-blue dichotomy in Parliament, maybe there’s a party who does.

Because, luckily :) there’s a democratic resurgence.
What do you make of this OIA where a few months ago a work plan was proposed to, "...address the significant and inequitable impacts of inadequate nutrition, inactivity and obesity" on health outcomes between the Ministry of Health, Te Whatu Ora and Te Aka Whai Ora?
https://www.health.govt.nz/system/files/documents/information-release/h2023028274_response.pdf
Great to have someone with nouse airing this stuff.