


Emergency Powers: [13] Appropriating the agency of medical experts.
From my April 2022 paper COVID-19 Emergency Powers: The New Zealand State, Medical Capture & the Role of Strategic Ignorance

Chapter 13
There is no doubt the New Zealand state expected genetic vaccine compliance across the nation, regardless of age-stratified risk. The COVID-19 Vaccine Immunisation Programme Service Standards stated
‘COVID-19 Vaccine has been secured for everyone in New Zealand/Aotearoa aged 12 years and over to receive the two doses they need to protect against COVID-19’
and the Medical Council of New Zealand declared that there was
‘no place for anti-vaccine messages’ or ‘ promotion of anti-vaccine claims’.
It mattered not to the Medical Council of New Zealand that vaccination historically prevented transmission and infection from an infectious disease; nor that the novel genetic vaccine technologies were provisionally approved because they lack full clinical trial data to confirm safety.
The ‘deviant’ doctors, through the insistence on applying the practice of informed consent (institutionalised in law, via the Belmont Report, the Code of Health and Disability Services Consumers' Rights) directly challenged government dogma that presumes all people should accept a provisionally approved, mRNA genetic vaccine, and then stepwise agree to vaccine passports.
Globally, these physicians further challenged the power of the New Zealand state when they discussed alternative treatment options which include multitarget medical and nutritional treatments from repurposed drugs with a long history of safe use. COVID-19, as with HIV/AIDs, is a complex disease requiring complex treatment protocols.
State institutions effectively expunged the personal agency of frontline medical personnel by exhorting doctors to conform; by focussing on cases rather than hospitalisation rates -
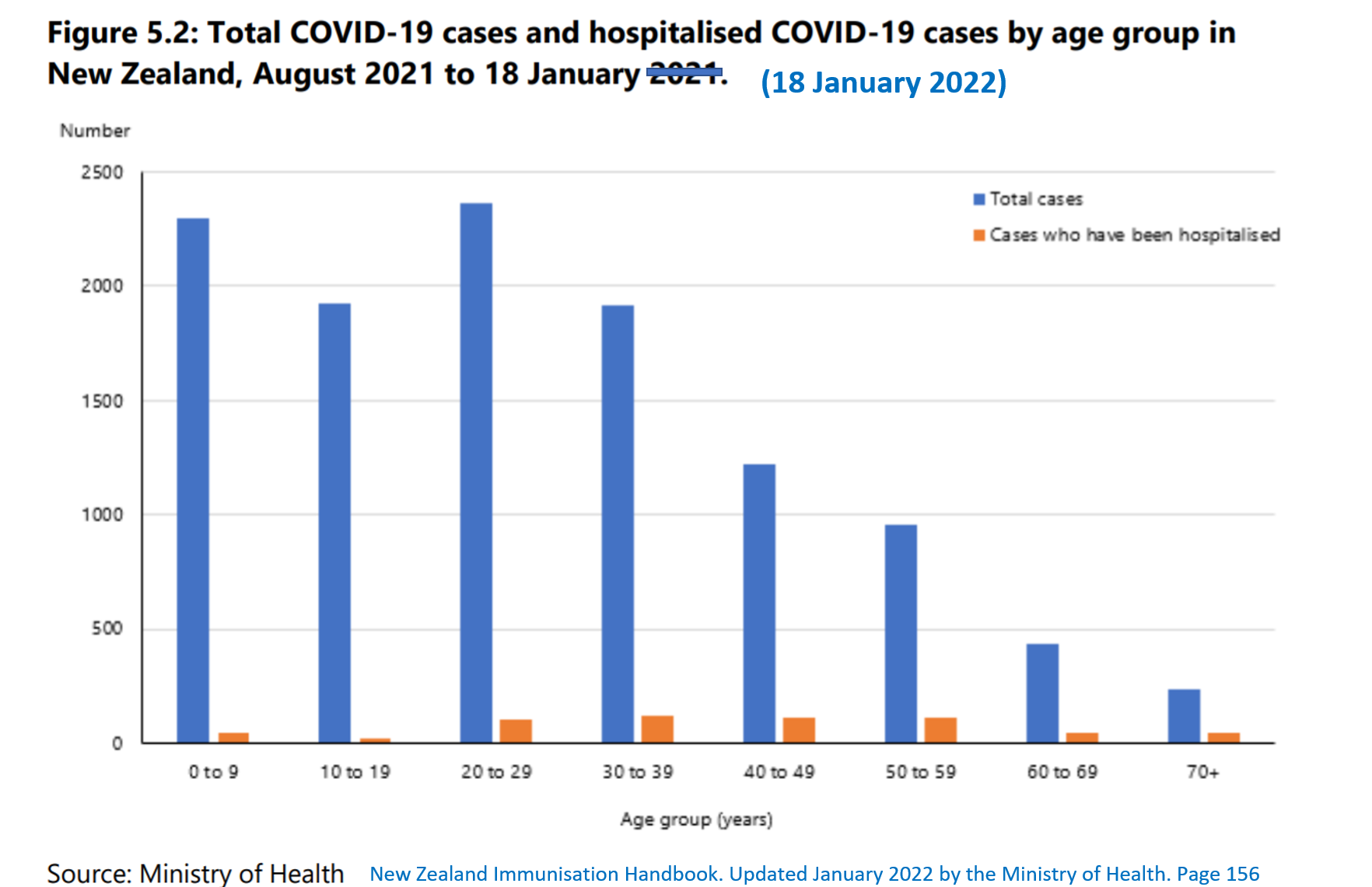
conflating doctors guidance with ‘personal beliefs’ ; ignoring mRNA gene therapy risk by age group; discouraging repurposed drugs that produce an integrated response to the complex pathologies present in COVID-19; and by ignoring nutritional and other lifestyle therapies, particularly useful to buffer lower-socioeconomic groups at greater risk of immune-related nutrient-deficiency.
What can be observed in New Zealand, is the power of the state in full roar. Cabinet, the Ministry of Health, Pharmac, MedSafe, the drafters of legislation, the funded media (and media watchdogs), the silent and compliant universities and the Medical Council of New Zealand. These institutions have effectively operated in concert to shepherd all to genetic vaccine compliance and produce and sustain ignorance and control the political narrative.
Agreements with the manufacturer further impeded transparency. Secret (commercial in confidence) government contracts with the mRNA genetic vaccine supplier made it difficult to understand what data was supplied in support of the technology. It remains unknown whether there is a potentially chilling effect arising from international trade agreements, such as the Comprehensive and Progressive Agreement for Trans-Pacific Partnership (CPTPP) should contracts be suspended.
Doctors dealing with complex conditions normally exercise personal agency, personal judgement in order to make the best decision for their patient. Conventionally, repurposed drugs, such as the antiviral Ivermectin, would be widely used in multiple scenarios, with doctors given latitude to make such decisions. However, COVID-19 clinical guidelines have steered clinicians away from such practices. 418 419
Ministry of Health (2021, Jul 9). Science Update.
Ministry of Health (2022, Feb, 4). Clinical Management of COVID-19 in Hospitalised Adults (including in pregnancy).
The state has never before restricted access to traditionally safe off-label use of an historically safe drug. Restrictions, policies and guidelines across government institutions can be observed to act in concert, and ultimately produce multiple forms of ignorance that place the public at risk of hospitalisation and death – because they remove agency and discretion from doctors.
The policies discussed in this paper render as precarious, judgements outside guidelines which are normally common in practice. The statements and warnings delivered by government institutions have produced a chilling effect across the health field. This institutional power has captured hospital medics, ambulance medics and medical practices through an overarching culture and instrumental policy that cannot judge and weigh risk differently – and respond to the needs of an individual patient - without risking the consequences of a report to authorities that may result in social, professional and/or political ostracism.
Narrowly derived, dictated protocols perpetuates a learned helplessness, a ‘nescience’ – that by restricting agency removes autonomy and learning in the practice of medicine. These protocols promote impotence and anxiety of ramifications should they step outside clinical guidelines and be reported to the MCNZ.
Medicine is a notoriously conservative profession, and the public shaming of the dissident medical doctors has been loud and clear. Radio New Zealand has led in describing doctors as ‘anti-vax’ (here and here and here) for expressing caution concerning the novel mRNA treatment and attempting to support patients that that were forced to have the genetic vaccine in order to secure their jobs.

These doctors had worked for decades in isolated rural communities.
Health providers normally struggle to get long term doctors in isolated communities.
Continue Reading: Emergency Powers: [14] Will the courts decide? here
References are available on the original PDF at TalkingRisk.NZ