
Reframing Risk. RedFlagging it. Regulatory loopholes & Provisional Consent
(B) The God trick. It's the company who sets the standard on what is efficacy - & controls the predominant data stream disclosing product risk (safety) & efficacy.

Part 2.
INTRODUCTION
Note: The H202106950 link to the Health.govt.nz, described in this OIA request, has since been removed by the Ministry. This document included New Zealand’s clinical evaluation of the Pfizer/BioNTech product, TT No. TT50-10853, Application ID 109400. This document does not appear to be anywhere on public facing sites.
Throughout COVID-19, legislation, rules and guidelines have been systematically applied to favour the deployment of the mRNA gene therapy. This substack REDFLAGS loopholes, which, while viewed separately appear logical, but viewed in sequence, rather like an orchestra, demonstrate how decision-making persistently shepherds governance cultures and decision-making processes to favour the industry sponsor, Pfizer.
These loopholes undermine the states fiduciary obligation to protect health. They exclude processes requiring independent review of the scientific literature; and instead shift evidence to favour that supplied by the industry sponsor. This institutionalises processing patterns that favour medical treatments, even in environments of pervasive uncertainty and doubt.
Attorney General David Parker’s fast-tracked one day overarching legislation did not contain a broad (ethical) principle requiring that health was protected over the pandemic period. Parker’s legislation focussed on transmission of infection, not infection or case fatality rate. Fear was based on infection risk. This set the tone for how risk would be addressed and responded to by the government.
Protection is a principle - it is a general and somewhat abstract. It overlaps with ethics, how and why do we draw attention and define danger, risk, what is right and wrong and how we take steps to prevent and protect individuals. Ethics tend to be closely associated with culture. This is why decision-making around health requires sunlight and democratic consensus in order to assist in making moral judgements around what protection infers.
Marie Hedlund articulates this well:
To be democratically justified, it is necessary that ethics expertise uses its clarifying expertise and provides different possible moral positions for the public and democratically accountable decision-makers to deliberate and decide upon.
What courses through the debate is of course, the idea that precaution might stymy progress, and that medical innovations equate with social and economic progress. Drawing attention to danger and risk contradicts these positivist framings.
The best way to assist industries with financial or political interest in the outcome, is to avoid issues of ethics and precaution - steering clear of moral hazard.
Instead, responsible officials, working with industry ‘stakeholders’, construct policy and legislation in such a way that establishes neatly constructed loopholes, through which the institution with the political and financial conflicts of interest can slip neatly through. The loopholes firstly, technocratise the process; secondly, prevent the public accessing data and thirdly promote ignorance relating to ethics and judgement.
In constructing these loopholes - which I REDFLAG throughout this document - officials may merely see themselves as getting the job done. Yet, such techniques have been refined for decades by large industries that seek to prevent uncertainty and doubt in the public or political sphere. The endgame of loopholes? To remove questions of risk and safety that might lead to withdrawal of their products from the market.
I consider that these processes reflect an erosion of democratic process. Parliament’s habit of fast-tracking morally questionable legislation included expansion of provisional consent to not just small groups but to the entire population. Was this the penultimate loophole of the Pandemic Campaign?
(A) LOOPHOLE ALERT: APPLICATION DOC SETS SCOPE
THE NOVEL GENE THERAPY PRODUCT
October 21, 2020. Regulatory Affairs Department, Pfizer New Medicine Application. Information released under the OIA, Ref: H202106950:
The product: a nucleoside-modified messenger RNA encoding the SARS-CoV-2 S-glycoprotein intended to provide immunisation against COVID-19 caused by the virus, SARS-Cov-2.
The Pfizer and BioNTech COVID-19 Vaccine is based on SARS-CoV-2 spike (S) glycoprotein antigens encoded in RNA and formulated in lipid nanoparticles (LNPs), referred to as COVID-19 Vaccine (BioNTech code number BNT162b2, Pfizer code number PF-07302048).
The RNA-based vaccine encodes a viral antigen which is expressed by the vaccine recipient and can elicit protective immune responses. Unlike live attenuated vaccines, RNA vaccines do not carry risks associated with infection. RNA-based vaccines are manufactured by a cell-free in vitro transcription process, which allows easy and rapid production and the prospect of producing high numbers of vaccine doses within a shorter time period than could be traditionally achieved with conventional vaccine approaches.
NEW MEDICINE APPLICATION
October 21, 2020. Regulatory Affairs Department, Pfizer. New Medicine Application. Information released under the OIA, Ref: H202106950 (31/162) :
This application seeks provisional registration of a new biological entity, BNT162b2 [mRNA], hereafter referred to as BNT162b2, under section 23 of the Medicines Act, for an RNA-based vaccine to prevent Coronavirus Disease 2019 (COVID-19) caused by the SARS-CoV-2 virus.
(1) REDFLAG- New Biological Entity - ‘active substance’
(Medsafe Guidelines 2020 p.12/66)
So it’s biological entity - biological active substance (also known as an active pharmaceutical ingredient, API). Medsafe recognised that this vaccine was a ‘higher-risk medicine’, stating:
This vaccine contains a new biological entity, so a data protection period will apply for 5 years from the date of Gazette (p.45).
Funny how they updated the guidelines in October 2020.
Firstly, it’s not the sort of biotechnology that comes under HSNO. As I’ve noted:
Pfizer approached the New Zealand Environmental Protection Authority (NZEPA) on the 29 th of January 2021 (APP204176) seeking confirmation (a Section 26 Determination) 245 that Comirnaty COVID-19 Vaccine (BNT162b2 [mRNA]) did ‘not meet the definition of an organism (nor of a genetically modified organism) and therefore cannot be considered a new organism under section 26 of the Hazardous Substances and New Organisms (HSNO) Act 1996. Three days later a staff assessment report was produced by the NZEPA recommending that BNT162b2 does not meet the definition of an organism in the Act, and therefore it cannot be a new organism for the purpose of the Act.
Right then. Higher risk, new biological active substance, but not biotech.
But, secondly, it is higher risk which sould trigger broader consideration, but it is approved as a vaccine. This is despite the fact that traditionally, vaccines did not involve a tech that contains the genetic instructions to produce an inflammatory protein inside the body in an uncontrolled way.
The box ticking of this new biological entity shifted the regulatory framework from being positioned as a biological or biotechnological product to a vaccine. It steered regulation down the vaccine approval path, but without long-term data, which would ensure the manufacturer had indemnity from potential harm.

(2) REDFLAG - to prevent disease not immunise against infection.
But it is a vaccine which is promised to prevent disease not prevent transmission of infection. This is an important distinction. Immunization is a process of inoculation to prevent infection, such as smallpox. Once inoculated with the smallpox virus the body would produce an immune response that would confer protection against infection. It would provide immunity.
COVID-19 is the disease is the series of symptoms that arise following infection by the respiratory coronavirus SARS-CoV-2.
Pfizer’s application did not promise immunity from infection. Over time vaccine narratives have switched from the narrower inoculation to prevent infection, to a broader prevention against disease.
This broadens the category of vaccine. A key strategy used by the pharmaceutical industry is to capture a wider range of symptoms listed under a disease category which then expands the market for a product.
(3) REDFLAG - consent manufactured on the basis of infection risk.
Most of the population were known to not be at risk of COVID-19 disease, from March 2020. This was definitely confirmed prior to this application, October 2020.
However government propaganda centred around a vaccine to prevent the spread of infection. This manufactured consensus for widespread acceptance in order to protect coworkers, whanau and the elderly. Prevention of transmission of infection was never an endpoint in the clinical trial.
There may be a fundamental disconnect here with the public’s knowledge of the traditional vaccines, for example the measles or smallpox vaccines to prevent transmission of infection. As I have previously outlined, the mRNA genetic vaccines are vastly different from traditional live attenuated virus or inactivated vaccines.
Yes, smallpox vaccines have been mandated. Bioethicist Professor Julie Ponesse has explained that analogies between smallpox and COVID-19 don’t hold up under scrutiny, and the court case that found for mandates for the smallpox vaccine in the USA, Jacobson v Massachusetts (1905) concerned markedly different facts:
‘Smallpox is highly virulent with an infection fatality rate more than thirty times greater than COVID-19. The average age of death from COVID-19 exceeds the national life expectancy, whereas smallpox preyed on the very young (one to five years) and middle aged (thirty to sixty years). Furthermore the smallpox vaccine was a ‘sterilizing’ vaccine', whereas the COVID-19 vaccines are ‘leaky’ meaning they don’t always protect recipients of the vaccine who are exposed to the virus and they permit recipients to be infectious. Furthermore, the virus that causes COVID-19 has been found to infect a wide range of animals, including bats, cats, minks, pangolins and wild deer, whereas smallpox could only spread through human contact.’ (p.40-41)
(4) REDFLAG - Regulatory Data Protection (RDP) period of 5 years.
As a biological entity, Pfizer gets an exclusive right to benefit from all the data produced in the pre-clinical and clinical trials. So for 5 years this data for a novel, high risk, biological genetic therapy gets hidden because the corporation went to considerable expense to produce the data.
This means there is no public scrutiny of the data. Commercial in confidence agreements are an important technique (loophole) used to prevent critical appraisal (that might lead to precautionary regulation).
(5) REDFLAG - massive conflicts of interest in Pfizer controlling data.
Noting that the cost of clinical trials are far outweighed by profit. Macrotrends state:
Pfizer annual/quarterly gross profit history and growth rate from 2010 to 2022. Gross profit can be defined as the profit a company makes after deducting the variable costs directly associated with making and selling its products or providing its services.
Pfizer gross profit for the quarter ending June 30, 2022 was $19.094B, a 60.41% increase year-over-year.
Pfizer gross profit for the twelve months ending June 30, 2022 was $62.976B, a 60.46% increase year-over-year.
Pfizer annual gross profit for 2021 was $50.467B, a 52.16% increase from 2020.
Pfizer annual gross profit for 2020 was $33.167B, a 0.96% increase from 2019.
Pfizer annual gross profit for 2019 was $32.851B, a 3.18% increase from 2018.
(6) REDFLAG - Higher risk medicine. But a vaccine status= lower hurdles
As we can see in the box below - BNT162b2 gene therapy is classified as a higher risk medicine.
February 2, 2021. OIA, Ref: H202106950 Extract from the minutes of the 109 th meeting of the Medicines Assessment Advisory Committee held in Wellington on 2 February 2021 commencing at 9:30am

But - the application is for a higher risk biological entity that is classified as a vaccine.
The disconnect (contradiction) may come from the fact that most vaccine rules and regulations reflect the fact that vaccines are traditional live attenuated virus or inactivated vaccines. They are considered less risky and they have a lower bar of data than biological or biotechnological products.
(7) REDFLAG - Vaccine with indemnity, but no long-term studies.
I have discussed the potential for long term chronic health conditions, including the potential for vaccine-associated enhanced disease risk here. This chart demonstrates the fast-tracking and and identifies some of the long term (chronic) health risks that could not be untangled in short time frames:

(8) REDFLAG - Vaccine status - no genotox/cancer studies required.
OIA, Ref: H202106950 (p. 34/162).
This loophole is rather magnificent.
None of the components of the BNT162 vaccines (lipids and RNA) are suspected to have genotoxic potential. In addition, no impurity or component of the delivery system warrants genotoxicity testing. Therefore, in accordance with the WHO guideline, no genotoxicity studies were performed.
RNA itself, and the lipids used in the BNT162 vaccines, have no carcinogenic or tumorigenic potential. Furthermore, according to ICH S1A, no carcinogenicity studies are required for therapeutics that are not continuously administered. Therefore, no carcinogenicity studies were performed.
I believe that traditional clinical trials for medicine require genotoxicity and carcinogenicity studies are undertaken. But for traditional live attenuated virus or inactivated vaccines this issues were considered not such a risk. This has not Jessica Rose has outlined the slight problem here.
(9) REDFLAG - Vaccines aren’t continuously administered. But boosters?
Ref: H202106950 (p. 34/162).
Furthermore, according to ICH S1A, no carcinogenicity studies are required for therapeutics that are not continuously administered. Therefore, no carcinogenicity studies were performed.
Let that sink in. Remember how the childhood vaccines were based on old school traditional live attenuated virus or inactivated vaccines, but BNT162b2 is contains the instructions for the spike protein to be produced inside the body.
The spike protein persists (here and here), and therefore potentially accumulates.
Yet traditional vaccines regulations/guidelines are based on a couple of injections in a short time period, not ongoing exposure.
For frontline health professions with high risk exposure to infectious disease, it has been convention for many years for staff to have serology tests to understand if they have pre-existing immunity, and then accept a range of vaccines to fill in the gaps where they are not immune. No such capacity was provided for mandated workers over 2019-2022 for COVID-19.
They were then (and are now) subject to continuous administration of the injection.
(B) LOOPHOLE ALERT: PROVISIONAL CONSENT GAMED
In the past year I have conflated provisional consent with an emergency situation. But this is incorrect. New Zealand did not reach a level of emergency. Deaths and hospitalisations following exposure to SARS-CoV-2 hadn’t triggered emergency status. Nor did New Zealand have an Emergency Use Authorisation (EUA) pathway.
Instead, New Zealand and Australia fast-tracked vaccine approvals through the provisional consent approval process (see (D) below). Australia’s review time frame for provisional consent was shortened from 255 days to 54 days.[2]

Provisional consent (PC) was a tool to get small batches of drugs over the line – consent would be approved on a restricted basis – to meet an urgent clinical need. As the judgement for Nga Kaitiaki Tuku Iho Medical Action Society Incorporated v Minister of Health & Others discusses, PC was introduced in 1981, with the caveat it would be applied for a ‘limited market’. PC could be applied for drugs that might not be ‘profitable if marketed’, or it could be applied when there was insufficient documentation. Rationale for PC included:
No one would want to see a handful of patients denied their treatment because the allotted 2 years had elapsed and some formalities had not been concluded.
In line with the pattern industry friendly guideline shifts that result in regulatory loopholes, in 1987 the Act was amended to permit the renewal of PCs.
This was why a gene therapy that encodes a viral antigen which is expressed by the vaccine recipient, could evade traditional, lengthy processes that established safety for new, products that were yet to be thoroughly tested across the population.
(10) REDFLAG - Provisional consent. Law change to favour a national roll-out of a novel gene therapy. Wow.
On February 2, 2021, the Medicines Assessment Advisory Committee (MAAC) unanimously recommended that a provisional consent be granted for a nine-month period, on that day Christopher James (Medsafe) granted provisional consent and the New Zealand Gazette published notification of provisional consent for use of the Pfizer Comirnity BNT162b2 vaccine for people 12 years and older. [8]
February 2, 2021. Approval was signed and published in The Gazette:
‘Provisional consent is to be granted for nine months to address an urgent clinical need.’
PROVISIONAL CONSENT: FOCUS ON 58 CONDITIONS
Provisional consent (see Section 23(1) Medicines Act) was contingent upon the manufacturer providing more information as data is produced and released. The New Zealand provisional consent approval specifies 58 conditions that the industry sponsor must comply with.
These conditions place language around renewal - as contingent upon the sponsor providing information.
The list of requirements included in the Gazette notice was detailed. The requirements put in place specific obligations that the New Zealand Sponsor had to undertake.
On February 5 2021, after provisional consent was granted, Dr Caroline McElnay, Director of Public Health communicated the COVID-19 Vaccine Technical Advisory Group (CV TAG) recommendations in a memo. The group noted a
‘relatively high prevalence of common side effects.’
The appendix did not include any advice to review the peer reviewed literature, but emphasised that the Sponsor, Pfizer should provide data from clinical trials, reports from other regulators and provide regular safety reports.
The basis for renewal was the sponsor fulfilling the conditions established in the Gazette notification. These conditions do not include:
Baseline levels of safety or efficacy.
Communication that the regulator will review the scientific literature to triangulate and confirm/refute industry claims.
The Risk Management Plan (RMP) doesn’t require that the scientific literature is reviewed to understand what scientists are reporting and identifying globally. Medsafe’s responsibilities regarding vaccine safety include the review of the scientific literature, but there doesn’t appear to be a dedicated page for the public to understand what reviews are being undertaken of the published scientific literature.
(11) REDFLAG - Urgent clinical need? Addressed by existing medicines.
Early treatments were identified (at least) by December 2020. I’ve discussed the New Zealand governments propaganda campaign produced a chilling effect that shepherded workers and the public towards the gene therapy. The propaganda campaign, and alliances with the New Zealand Medical and Dental Council acted in concert to silence critical dissent; eject repurposed antivirals from the national narrative by imposing strict guidelines around COVID-19 treatment; ignore early treatment; and target and shame doctors.
(12) REDFLAG - Pro-gene therapy NZMC outside of OIA request jurisdiction.
Doctors that have been critical of risk, remain under gag orders in New Zealand in August 2022.
Doctors gag orders and threats to withdraw doctors licences take place through the New Zealand Medical Council which have demanded that doctors are not critical of the mRNA gene therapy. However, it is impossible to conduct OIA requests to understand the patterns of pharmaceutical industry influence. This may include longstanding relationships with larger associations such as the International Association of Medical Regulatory Authorities and their relationships with the pharmaceutical industry. This can include relationships with the World Health Organization who have close ties to industry sponsors.
PROVISIONAL CONSENT: EASY RENEWAL
The provisional consent for the 12 years and above mRNA product was renewed on November 3, 2021.

PROVISIONAL CONSENT: CHILDREN AGED 5-11 YEARS
Provisional consent for the age 5-11 years dose was granted December 16, 2021, and valid until November 3, 2023.

PROVISIONAL CONSENT: A LIMITED NUMBER OF PATIENTS
In April 2021, Nga Kaitiaki Tuku Iho Medical Action Society Incorporated (KTI) filed for judicial review in the High Court,[4] challenging the legality of the s23 provisional consent approval, and filed an application for interim orders. The plaintiff claimed there was an error of law as the ‘limited number of patients’ stipulated in the Act was not identified, and that the rollout would be unlawful (p.15/24). The plaintiff was concerned about the implications of population-level treatment, particularly for mandated workers.
In the May 18 judgement, it is interesting that Judge Ellis’ deliberations were partially based on her trust of the public health risk formulated by actors charged with administering New Zealand’s public health system. In particular, in her consideration of the public health benefit arising from vaccination; she stated a belief that
‘vaccination is not, and will not be, compulsory for the vast majority of the New Zealand public’;
while noting that informed consent will otherwise be sought and obtained before any act of vaccination.
In the judgement handed down on May 18, 2021, Judge Ellis concluded
[75] I have also found that it is reasonably arguable that the provisional consent granted to the Comirnaty vaccine was ultra vires s 23 of the Act, and I would urge the Crown now to consider that question carefully. For now, I decline to exercise my discretion to grant the interim orders sought. The adverse public and private repercussions of doings so are too great, by some very considerable margin.
[76] The application for interim orders must therefore be declined.
On the 18th of May the Hon Andrew Little announced that S 23 of the Medicines Act would be amended the next day. On the 19th of May the Attorney-General concluded, without receiving the final version of the Medicines Amendment Bill, that
The Bill appears to be consistent with the rights and freedoms affirmed in the Bill of Rights Act. In reaching that conclusion, we have considered the consistency of the Bill with s 10 (right not to be subjected to medical or scientific experimentation) and s 27 (right to justice).
(13) REDFLAG - Parliament expedited legislation change in 1 day.
The Medicines Amendment Bill was introduced (Bill 41–1). First reading (skipped), second reading, committee of the whole House, and a third reading (skipped) on May 19, 2021. Royal assent was granted May 24, 2021.
The text requiring that provisional consent granted on a restricted basis for the treatment of a limited number of patients, was removed from the legislation.

Nga Kaitiaki Tuku Iho Medical Action Society Incorporated (the Plaintiff) and Sue Grey, the lawyer for the Plaintiff, released a documentary video, one year later, describing this experience, the enormous public support and attendance in the New Zealand High Court. The documentary discusses some of the underpinning ethical and legal issues arising from this process. It’s worth watching.
(14) REDFLAG - No ‘line of site’ to the company fulfilling the conditions.
Principles of law require transparency and accountability. Yet company information and decision-making have been opaque and difficult to access. This again, acts as a loophole because such activities positively bias the industry sponsor. In the documentary video and in an Open Letter dated March 31, 2021, lawyer Sue Grey noted that provisional consent was subject to the sponsor fulfilling these 58 conditions. Grey noted
No information is available for the public or their advisors to assess compliance with these conditions.
Searches on Medsafe, the Unite Against Covid site and on the Ministry of Health do not bring up clear data to demonstrate timelines and evidence to demonstrate transparently that these were fulfilled. However due to the regulatory data provisions this information remains undisclosed (see Loophole Alert 4 RDP).
Provisional consent is the loophole that has ensured the novel gene therapy product could evade long term and wide ranging safety trials and bypass broader, deliberative scrutiny around efficacy.
Nine months later, when the consent was renewed, it was able to be renewed because the manufacturer had complied with the conditions by sending in the information that was requested. Medsafe Group Manager Chris James explained that:
‘Pfizer has met all obligations required to date by the conditions of the provisional approval granted in February this year. This included providing additional data about the clinical trials and vaccine monitoring.’
‘The remaining conditions relate to ongoing supply of clinical trial data, ongoing requirements for monitoring the use of the vaccine globally, specific batch test results for vaccine supplied in New Zealand, and reporting these to Medsafe on request.
Safety and efficacy were not publicly discussed.
The availability of information is crucial for all forms of accountability, but transparency, or the widespread availability of information, is essential to market, peer, and reputational accountability, as well as to the internal workings of democratic accountability in states which play a supervisory role.
Medsafe’s website includes links to the gazette notice, data sheets etc.
Yet there is no line of site which helps the public understand Pfizer’s timeliness and capacity to fulfill the 58 obligations, which have now been whittled down to 12 obligations relating to the provisional consent for children.
(15) REDFLAG - No baseline trigger level to prevent renewal or revoke consent.
In law: ‘The criterion 'the public interest' is a yardstick of indeterminate length.’
But apparently in the New Zealand governement - the corporate interest is now a yardstick of indeterminate length.
There was no baseline trigger established from the outset, when adverse events or deaths were recorded in the white, grey or published literature at sufficient levels that would stop the injections. Instead, provisional consent was directly related to the manufacture complying with the conditions set by the regulator, Medsafe. Therefore, when experts state
‘there's lots of post-market evaluation, as new information comes to light… so it's definitely been a fabulous process’[3] –
the information and evaluation arrives via the industry sponsor. No baseline trigger level of harm was separately established by regulatory authorities.
PROVISIONAL CONSENT: WHAT IS EFFICACY?
Efficacy of a medical drug is generally recognised as the
maximum response achievable from a pharmaceutical drug in research settings
Research results suggest the
drugs capacity for sufficient therapeutic effect or beneficial change in clinical settings.
From the commencement of regulatory processes to authorise the BNT162b gene therapy, it was Pfizer who maintained control of how efficacy would be recognised and defined.
Efficacy has been left out of the renewal discussion, but the decision whether provisional consent should be revoked has been outside any public discussion.
(NB. It’s evident that new information can be supplied as a notice deposited under Section 24. The Medsafe website contains no public information to support that this has occured).
PROVISIONAL CONSENT: CONDITIONS TO REVOKE?
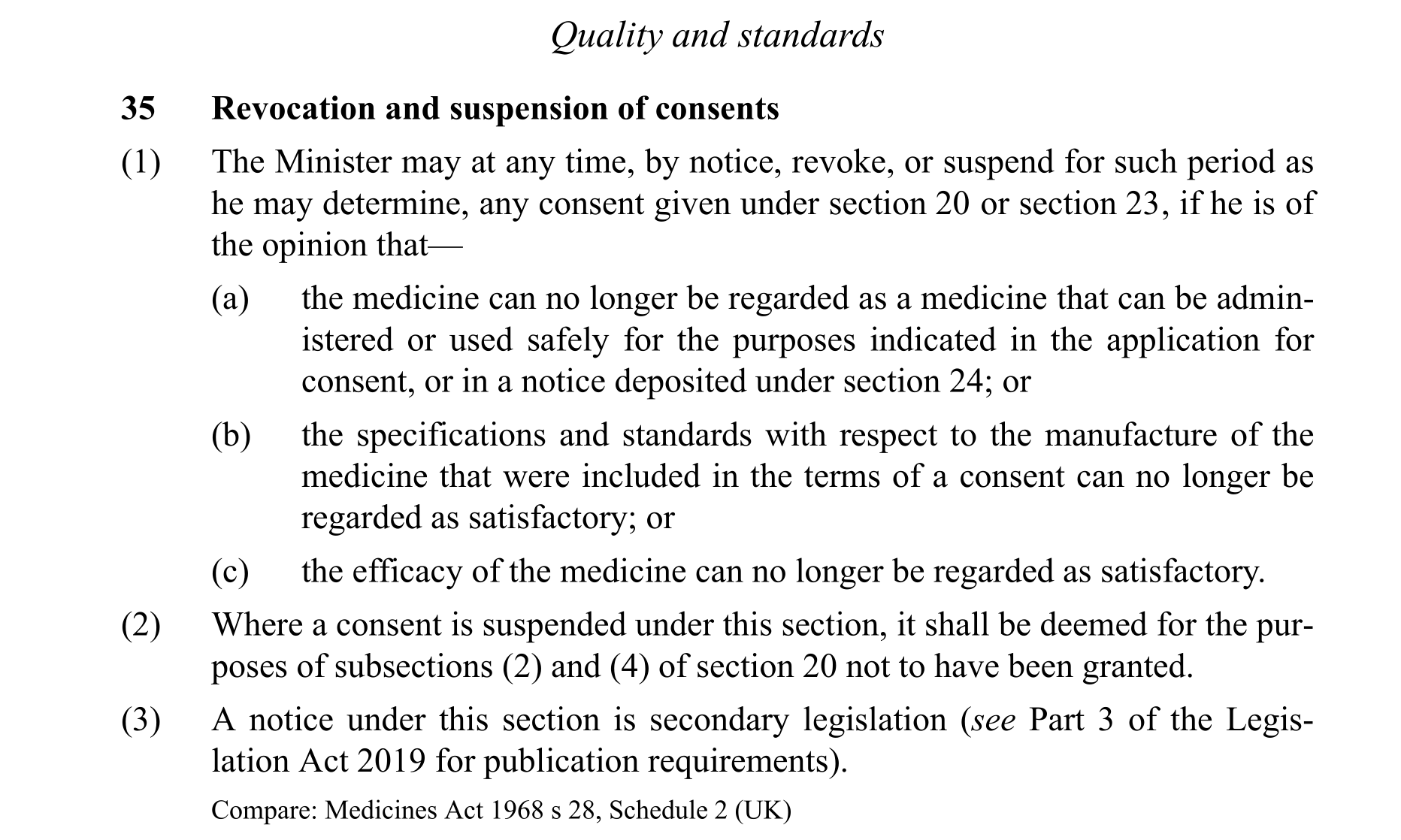
Note the way Section 35 is structured.
Consents can be revoked or suspended (Medicines Act, S35), if:
a. The medicine cannot be regarded as a medicine that can no longer be administered or used safely for the purposes in industries’ application for consent;
b. If the specs in the application for consent are no longer regarded as satisfactory;
c. If the efficacy is no longer satisfactory
Ref: Application for consent (p.31/162) : New Medicine Application. COVID-19 Vaccine (BNT162b2 [mRNA]) concentrated suspension for injection, 30 µg/0.3 mL, 0.45 mL multi-dose vial. Application made by the Regulatory Affairs Department Australia/New Zealand Pfizer Australia.
Administration and use
Let’s attempt to examine what obligations are put in place by 35(1)(a) and 35(1)(c).
If we look at the New Medicine Application, what did the application for consent actually say was the ‘purpose’ of the new biological entity (but not a new organism)?
a. The medicine cannot be regarded as a medicine that can no longer be administered or used safely for the purposes in industries’ application for consent;
Purpose: intended to provide immunisation against COVID-19 - i.e. Proposed Indication: Active immunisation against COVID-19 disease caused by SARS-CoV-2 virus in individuals aged 16 years and over. (p.30/162)
Purpose is for immunisation. Where is ‘active immunisation against disease’ defined? (See REDFLAG (2)).
b. If the specs in the application for consent are no longer regarded as satisfactory. Well. The specs changed, then industry had to apply and send in a load of data that was hidden from the public.
c. If the efficacy is no longer satisfactory - see below.
(C) LOOPHOLE ALERT - PIVOTAL TRIAL DATA SETS SCOPE
HIGH RISK PRODUCT BUT DECISION-MAKING BENDS TO THE SPONSOR
January 2021. Medsafe’s Clinical Evaluation contained a wealth of contradictions that demonstrated that they knew that severe disease risk was limited to populations, and that efficacy of the novel mRNA genetic technology beyond a month or so was not known. The product was a completely new technology, and the clinical trial data demonstrated wide-ranging side effects.
Theoretically, the novel mRNA genetic technology - a biological active substance (also known as an active pharmaceutical ingredient, API) - which instructed the human body to reproduce an antigen, a spike protein, should always have been restricted to narrow groups of at-risk people.
The evaluation’s Benefit Risk Assessment acknowledged that the respiratory virus was a ‘health hazard, especially for the elderly as well as people with comorbidities’ and that there were ‘relatively low mortality rates associated with the resulting disease, COVID-19’. The ‘benefit’ was based on reduction of symptomatic COVID-19 between 1 and 2 months after the second dose, with 95% effectiveness and no knowledge on how long ‘protection’ lasted. This 95% claim, based on pre-Delta data and echoed by Judge Ellis [38] in her May judgement. Judge Ellis also noted
38(c) Key to the benefit-risk balance was the probability of exposure to COVID-19, as well as its mortality and morbidity burden. The full picture of the benefit-risk balance was not available because of the data limitations. Nevertheless, a provisional consent was appropriate in light of the high clinical need, the quickly increasing experience with the vaccine, and the expectation of further data around April 2021.
The earliest clinical trials demonstrated that vaccinated people could also be symptomatic (i.e. the vaccine was not sterile). The efficacy for protection against severe disease (66%) was based on data … 7 days after the second dose. It was not known whether the product protected against severe disease, for a respiratory virus where only risk of morbidity and mortality was with ‘elderly as well as people with comorbidities’.
…and 21% of participants in the trial had an adverse event following administration.
Has the age stratified mortality and morbidity burden been released? I don’t believe so. Let’s look see if I can make sense of the processes…
APPLICATIONS & EVALUATIONS - PRIMARY EFFICACY ENDPOINT
October 21, 2020. Regulatory Affairs Department, Pfizer New Medicine Application. Information released under the OIA, Ref: H202106950:
The Application described the shortened study periods:
The phase 1 study (in Germany, BNT162-01) with 15 participants, demonstrated participants could tolerate the established dosage level.
The pivotal study : Phase 2/3, study C4591001 was designed to evaluate the safety, efficacy and immunogenicity of BNT162b2 in over 30,000 participants aged ≥18 years of age.
October 21, 2020. Pfizer letter did not confirm efficacy, instead efficacy would be based on November 2020 information (OIA, Ref: H202106950 ).
‘Pfizer will submit an initial dossier based on interim analysis of Study C4591001, in which efficacy is demonstrated, and will submit the final analysis of efficacy, in addition to safety data, when available, as agreed with Medsafe.’ (p.34/162)
November 13, 2020. Pfizer submits a new medicine application (ID 109400) for a
a nucleoside modified messenger RNA (modRNA) vaccine: the Pfizer-BioNTech COVID-19 Vaccine (BNT162b2 30 µg): Comirnaty (COVID-19 mRNA Vaccine).
December 4th 2020. Medsafe receives Pfizer’s Final Analysis Interim Report with a November 14 2020 data cutoff (the 2,033 page report appears to have been supplied 04-Dec-2020. OIA, Ref: H202106950 90/162).
The New Medicine Application and Interim Report supplied by Pfizer are not available to the public.
January 2021 (some time). Medsafe Clinical Evaluation of Study C4591001, was released signed by the ‘evaluator’ (Chris James of Medsafe?), (TT Number TT50-10853; Application ID 109400) (pp.86-100)
Redacted: pages 6-46; 46-49; 75-79.
January 28, 2021. Medsafe Medicine Evaluation Non-Clinical Studies. File Number TT50-10853. (pp.111-115)
Redacted pp.6-57
U.S. and European analyses of Study C4591001 are available:
European Medicines Agency (EMA) 2021, Feb 19. Assessment report. Comirnaty Common name: COVID-19 mRNA vaccine (nucleoside-modified). Procedure No. EMEA/H/C/005735/0000. EMA/707383/2020 Corr.1*1
(16) REDFLAG - Efficacy was only ever based on 170 cases after 7 days.
The final efficacy analysis occured when 170 cases in total were reached, 7 days after the second dose. The result, a total of 8 cases following BNT162b2 and 162 cases of infection following placebo.
The date for data cut-off for the final efficacy analysis was November 14, 2020, when a total of 170 confirmed COVID-19 cases were accrued. (FDA p.17/53)
The FDA provides a little more clarity on study C4591001 endpoints (6/53):
The primary efficacy endpoint is incidence of COVID-19 among participants without evidence of SARS-CoV-2 infection before or during the 2-dose vaccination regimen.
Vaccine efficacy for the primary endpoint against confirmed COVID-19 occurring at least 7 days after the second dose was 95.0% with 8 COVID-19 cases in the vaccine group compared to 162 COVID-19 cases in the placebo group.
First primary endpoint: COVID-19 incidence per 1000 person-years of follow-up in participants without serological or virological evidence of past SARS-CoV-2 infection before and during vaccination regimen – cases confirmed ≥7 days after Dose 2
Second primary endpoint: COVID-19 incidence per 1000 person-years of follow-up in participants with and without evidence of past SARS-CoV-2 infection before and during vaccination regimen – cases confirmed ≥7 days after Dose 2
Secondary Efficacy Endpoints Study C4591001 has secondary endpoints based on different approaches to COVID-19 case evaluation criteria as follows:
COVID-19 confirmed at least 14 days after Dose 2: COVID-19 incidence per 1000 person years of follow up in participants either (1) without or (2) with and without serological or virological evidence of past SARS-CoV-2 infection before and during vaccination regimen – cases confirmed ≥14 days after Dose 2
Severe COVID-19: incidence per 1000 person-years of follow-up in participants either (1) without or (2) with and without evidence of past SARS-CoV-2 infection before and during vaccination regimen – cases confirmed either (1) ≥7 days after Dose 2 or (2) ≥14 days after Dose 2
MEDSAFE EVALUATION: A NEW MEDICINE APPLICATION
That interim analysis, Pfizer’s Final Analysis Interim Report was supplied November 13, 2020, with a ‘safety population’ (H202106950 93/162) of N~38,000 with medium follow-up of two months.
Medsafe’s Clinical Evaluation released January 2021 noted that 21% of BNT162b recipients experienced an adverse event (p.93/162):
AEs judged to be related to vaccination were noted in 21% of BNT162b recipients vs 5% in the placebo group.
Adverse events more commonly reported in the 18-55 age group. The Medsafe evaluator noted that
· At this stage, there is limited evidence of protection against severe disease.
· There is no long-term safety follow-up information.
· Vaccine prevention of asymptomatic infection and disease transmission has not been established
Prevention of severe disease was 66.4%. This data was based on 1 person in the vaccinated group and 3 people in the placebo goup. Therefore it could be claimed that:
estimated efficacy against severe COVID-19 occurring at least 7 days after dose 2 was 66.4% (95% CI: -124.8%; 96.3%). (p.95/162)
At that date the unnamed evaluator stated (p.91/162)
follow-up data is only available for about one to two months. Therefore there is uncertainty about how long protection will last. In addition, the number of cases of symptomatic COVID-19 in subgroups of the study population is often low. There is thus uncertainty regarding efficacy in people of Polynesian and Asian ethnicity.
The pivotal study for this application is the Phase 2/3 Study C4591 001. At the earliest, it is from April 2021 that updated efficacy estimates regarding longer duration of vaccine protection are expected to become available.
It is not clear that the April estimates concerning ‘longer duration’ ever surfaced in a timely manner. Therefore, when provisional consent was granted efficacy was based on 7 days. This is where the efficacy endpoint remained
For participants without evidence of SARS-CoV-2 infection before and during vaccination regimen, from 7 days after the second dose, there were the following cases of symptomatic laboratory-confirmed COVID-19 of any severity;
· 8 (out of 18,198; 0.04%) in the BNT162b2 group and
· 162 (out of 18,325; 0.9%) in the placebo group
For the other co-primary efficacy endpoint, VE against confirmed COVID-19 in participants with or without evidence of SARS-CoV-2 infection was 94.6% (with 9 and 169 cases in the BNT162b2 and placebo groups respectively). In the elderly, participants ≥65 years of age with or without prior evidence of SARS-CoV-2 infection, VE was 94.7% (corresponding to 1 case in the BNT162b2 and 19 in the placebo groups).
From January 2021 it was known that symptomatic COVID-19 would occur in the BNT162b2 treatment group. It was also recognised that frail elderly groups could die following exposure, as a Norway study demonstrated.
Another issue concerns the mystery of some 200 people that were excluded from efficacy populations due to ‘protocol deviations’ on or prior to 7-14 days after dose 2. (See FDA doc 18/53).
(17) REDFLAG - Medsafe had the guts to say they couldn’t recommend consent.
In the Medsafe evaluation analysis (supplied via OIA request H202106950 p.76/162))
Due to the unresolved concerns and additional quality, safety and efficacy data to be provided at the time of completion of the evaluation, Medsafe is unable to recommend that this product be granted consent.
We can see that the application was transferred to the Medicines Assessment Advisory Committee (MAAC) on January 28 (p.116/162):
Medsafe is unable to recommend that the Minister’s delegate grant consent to the distribution of the product.
You are therefore asked to administer the recommendation that the Minister’s delegate refers this application to the Medicines Assessment Advisory Committee (MAAC) for consideration.
This was discussed by Sue Grey in the documentary as the information was in the documents released under the OIA. Judge Ellis judgement also showed the process of downwards delegation, from the Minister to the Director-General of Health to Mr Christopher James, the Group Manager of the New Zealand Medicines and Medical Devices Safety Authority (Medsafe).
mRNA VACCINE – PREVENTION OF SEVERE DISEASE AND DEATH?
From the commencement, the protection against severe disease was limited. The 66.4% claim appears, to me, misleading due to the low numbers.
(18) REDFLAG - 35,000 participants. Meaningful prevention of severe COVID-19? No.
The Medsafe Evaluation noted:
‘Severe’ confirmed COVID-19 meant that subject had in addition to the confirmed Covid-19 (for example) at least; severe systemic illness (eg RR ≥30 breaths per minute); or needing high-flow oxygen, or admission to an ICU; or death.
Severe disease was noted in one case of the vaccinated group and 3 cases in the placebo group. Although at this stage of the study’s follow-up, only about 1% of placebo subjects have developed symptomatic COVID-19, severe disease was not common (about 2% of those with symptomatic disease had severe disease; 3 out of162). (p.92/162)
Pfizer’s Final Analysis Interim Report had stated that severe disease was observed in one case of the vaccinated group and 3 cases in the placebo group. Therefore, the estimated efficacy against severe COVID-19 occurring at least 7 days after dose 2 was 66.4%. (p. 95/162.)
The Thomas et al 6-month trial data (p.14/18) demonstrated only 1 severe event in the BNT162b2 group, while there were 29 in the placebo group.
(19) REDFLAG - 6-month trial data: BNT162b2 1 severe event; placebo 29 events.
mRNA VACCINE - DEATHS FOLLOWING ADMINISTRATION
Adverse events led to twice as many withdrawing in the vaccine group (0.2% vs 0.1%)
The Medsafe January evaluation did not discuss the deaths. Historically, in the USA, five unexplained deaths would result in a black-box warning, while 50 deaths would result in withdrawing a drug.
The December 2020 FDA report noted (p.41/53):
A total of six (2 vaccine, 4 placebo) of 43,448 enrolled participants (0.01%) died during the reporting period from April 29, 2020 (first participant, first visit) to November 14, 2020 (cutoff date). Both vaccine recipients were >55 years of age; one experienced a cardiac arrest 62 days after vaccination #2 and died 3 days later, and the other died from arteriosclerosis 3 days after vaccination #1.
(20) REDFLAG - Public roll-out: 1223 deaths reported globally by February 4th.
A February 4 2021 post-marketing event report from Pfizer recorded 1223 deaths following injection with BNT162B2 in the wider global community.

The timing is remarkable. It was 2 days after provisional consent was granted.
(21) REDFLAG - 21 BNT162B2 deaths in clinical trials by March 13, 2021
A May 2021 FDA report noted (p.23/30).:
From Dose 1 through the March 13, 2021 data cutoff date, there were a total of 38 deaths, 21 in the COMIRNATY group and 17 in the placebo group. None of the deaths were considered related to vaccination.
Six month trial data was published with the release of the Thomas paper, November 4 2021 (before widespread mandates), and detailed in the Appendix.[7] Fifteen people died in the BNT162B2 group and fourteen in the placebo group.
At 6 months the trial claimed a 91.6% efficacy against placebo. This trial no. NCT04368728. opens in new tab. ‘randomly assigned 44,165 participants 16 years of age or older and 2264 participants 12 to 15 years of age to receive two 30-μg doses, at 21 days apart, of BNT162b2 or placebo.
The FDA permitted Pfizer to terminate the BNT162B2 study after 6 months, and then offered the vaccine to the placebo recipients, muddying the trial. The trial end points were vaccine efficacy against laboratory-confirmed Covid-19 and safety, which were both evaluated through 6 months after vaccination.
(22) REDFLAG – 6-month trial data: BNT162b2 15 deaths, placebo 14 deaths.
The potential for the vaccine to prevent severe COVID-19 after 6 months was as follows
First severe COVID-19 occurrence after dose 1 = Efficacy: 96.7 (80.3, 99.9) (Appendix 15/18)
· BNT162b2 1 person 8.439 (22,505)
· Placebo 30 people 8.288 (22,435)

(23) REDFLAG - How little data reviewed by October 2021
Even though the general population possible expected ongoing review of the safety and efficacy, perhaps discussions relating back to trial data, but hasn’t occurred. OIA request H202111774 is possibly the simplest vehicle with which to understand this.
“any and all minutes taken of meetings held by Medsafe pertaining to efficacy and clinical safety issues surrounding the Pfizer clinical trials of BNT162b2 mRNA COVID-19 Vaccine. I am specifically interested in Medsafe's independent analysis and appraisal of the above mentioned trials.
I would also like copies of any and all correspondence between Medsafe and the COVID Vaccine Technical Advisory Group pertaining to any and all safety concerns regarding BNT162b2. These concerns include but are not necessarily restricted to the clinical trial design; the exclusion of subjects from both the placebo and treated groups in the analysis of published data (N Engl J Med. 2020; 383: 2603-2615; FDA website); the use of diseasespecific endpoints instead of "all cause mortality and morbidity"; and what advice was given.”I would also like copies of any and all correspondence between Medsafe and the COVID Vaccine Technical Advisory Group pertaining to any and all safety concerns regarding BNT162b2.’
No data was held post February 2021. So no discussions.
(24) REDFLAG - Officials knew variants were already mutating at spike.
OIA request H202106950 p.64 shows us that the Ministry of Health Science and Technical Advisory Group (STAG) wondered about the SARS-CoV-2 virus strains and the implications for COVID-19 vaccines. Paragraphs discussing this knowledge appear to be redacted. On January 15, Chris James asked Ian Town and the Science and Technical Advisory (STA) team for evidence of increased transmissability of the ‘UK variant’ (p.101-110) and 50% increased transmissability of the Alpha variant was discussed.
Alpha variant B.1.1.7 was 1.5 times more transmissable. By January 2021, this variant, with 17 mutations was (globally I believe) responsible for 86% of infections. In February 2021, Wang et al. 2021 discussed that Beta variant B.1.351, which contained 9 spike mutations. Delta B.1.617 contained 9 spike mutations.
A recent paper by Zhan et al 2022 provides a timeline:

By July 2021 it was known that viral loads for Delta were 1000x higher than the 2020 strains. Regulators continued to base efficacy on identified case levels 2 weeks after the second dose for the Delta strain. The vaccine efficacy was not based on reduction of viral loads.
Pfizer had this data October 21, 2020, when they sent their first letter through that indicated more efficacy data would come through in the November Interim Report.
(25) REDFLAG - NO BIODISTRIBUTION STUDIES ON SPIKE PROTEIN
(Update May 2023.) While there was ample evidence the spike protein and the lipid nanoparticles circulated beyond the injection region, I had never realised that biodistribution studies were not undertaken to understand how far spike would travel. We now understand it translocates across the body, into the brain and across the placenta into the fetus.
New knowledge on risk simply isn’t considered
Is the modified spike protein a super antigen – is it more pathogenic than the SARS-nCoV-2 viral spike? Remember that loophole – or our tendency to approximate risk – of equivalency? Some scientists are concerned, just not regulatory scientists.
The Department of the Prime Minister and Cabinet (DPMC) has been tracking cases, hospitalisations and deaths and comparing them with three scenarios developed by COVID-19 Modelling Aotearoa. But of course, no policy paper held with the DPMC ever discusses deaths and harm from the gene therapy. It’s taboo.
As of January 27, 2022, the updated risk management plan (drafted, I believe by the vaccine manufacturer) makes no connection between the published literature and risk. It’s entirely based on sourcing data from the producer. Provision of the risk management plan is a condition of provisional consent.
The RMP details important risks of Comirnaty, how these risks can be minimised, and how more information will be obtained about Comirnaty's risks and uncertainties (missing information).
Over time, the RMP is updated as more information becomes available, including any new risks or changes to current ones. This RMP update was made in conjunction with the extension of the indication to children 5 to 11 years of age.
It’s not just me that is curious about how safety is navigated for an experimental gene therapy. We can see that others, whose curiosity and frustration has led to their OIA request FYI account being suspended, are curious also.
The validity of the hidden data is central to states’ claims for mandates. The legitimacy of 7 day efficacy data - is what the provisional consent is based around. The RMP is the mechanism that supposedly assures the public that actions are taken to manage risk.
Medical mandates have been found by New Zealand courts to be justifiable.
The god trick
The pretence, or performance of seeing everything from nowhere, that science, governing bodies, the surveillance state - could have infinite vision and that this could somehow be based on objective science (that would be best for everybody), produces what Donna Harraway described as the ‘god trick’.[1]
[1] Haraway, D. 1988 Situated Knowledges: The Science Question in Feminism and the Privilege of Partial Perspective. Feminist Studies, 14:3 (Autumn, 1988), pp. 575-599. https://wrdtp.ac.uk/wp-content/uploads/2021/01/HARAWAY-situated-knowledges.pdf
[2] Bathgate, S. March 17, 2021.Fast And Fabulous: How The COVID-19 Vaccines Got Approved So Quickly. https://www.medicalwriters.org/blog/fast-and-fabulous-how-the-covid-19-vaccines-got-approved-so-quickly/
[3] Bathgate, S. March 17, 2021.Fast And Fabulous: How The COVID-19 Vaccines Got Approved So Quickly. https://www.medicalwriters.org/blog/fast-and-fabulous-how-the-covid-19-vaccines-got-approved-so-quickly/
[4] NGA KAITIAKI TUKU IHO MEDICAL ACTION SOCIETY INC v MINISTER OF HEALTH & ORS [2021] NZHC 1107 [18 May 2021] https://forms.justice.govt.nz/search/Documents/pdf/jdo/b1/alfresco/service/api/node/content/workspace/SpacesStore/e8d47bc3-10dd-4ef9-ad96-5162f8f12f37/e8d47bc3-10dd-4ef9-ad96-5162f8f12f37.pdf
[5] Mollocana-Lara EC. Et al. 2021. The infinite possibilities of RNA therapeutics. Journal of Industrial Microbiology and Biotechnology, 48, 2021, https://doi.org/10.1093/jimb/kuab063
[6] Heinemann, JA, et al. 2021. Differentiated impacts of human interventions on nature: Scaling the conversation on regulation of gene technologies. Elem Sci Anth , 9: 1. DOI: https://doi.org/10.1525/elementa.2021.00086
[7] Thomas, S.J. et al. (2021). Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. NEJM. 385, 1761-1773 https://doi.org/10.1056/NEJMoa2110345 Adverse Events Page 6.
Thomas et al 2021 Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. Supplementary Appendix Table S4 https://www.nejm.org/doi/suppl/10.1056/NEJMoa2110345/suppl_file/nejmoa2110345_appendix.pdf
[8] NGA KAITIAKI TUKU IHO MEDICAL ACTION SOCIETY INC v MINISTER OF HEALTH & ORS [2021] NZHC 1107 [18 May 2021] https://forms.justice.govt.nz/search/Documents/pdf/jdo/b1/alfresco/service/api/node/content/workspace/SpacesStore/e8d47bc3-10dd-4ef9-ad96-5162f8f12f37/e8d47bc3-10dd-4ef9-ad96-5162f8f12f37.pdf