


Cancer and the evidence base for treatment (1).
Why is there so little research on diet and cancer when there is so much evidence for diet as a key factor driving cancer? It's political!

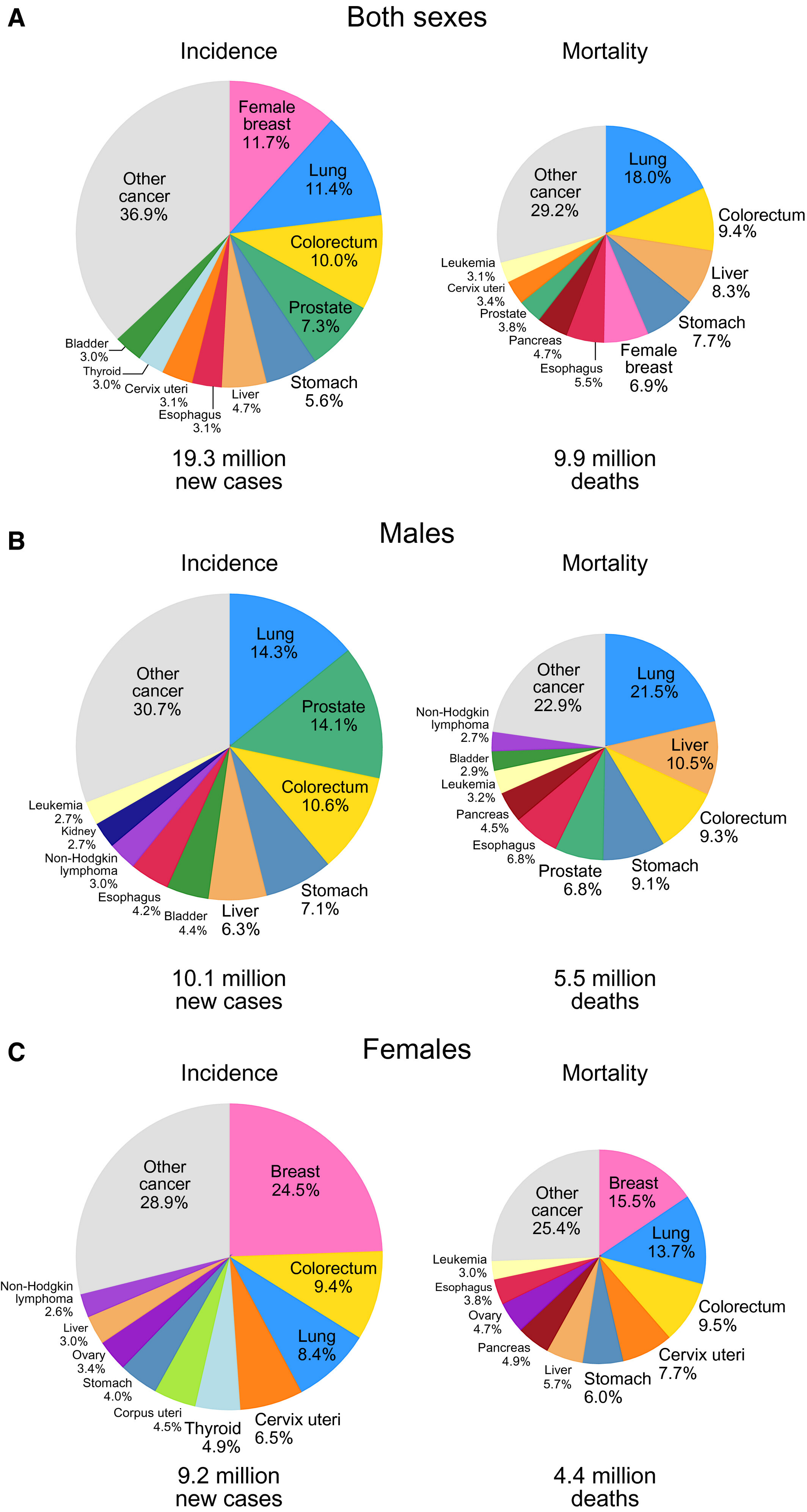
Cancer is engulfing us. In the US and UK, it is predicted that 1 in 2 people will be diagnosed with cancer. Cancer is the leading cause of death in the world. The top 10 cancer types account for >60% of the newly diagnosed cancer cases and >70% of the cancer deaths. We are told that cancer survival rates are up, - but what does that mean in real time?
More people are living longer than 5 years after being diagnosed. So - more people get cancer, and more people get treated. What does that tell you about the long haul? Recurrence? Quality of life? Not so much.
Assurances that treatments increase cancer survival statistics override the fact that more and more people have years lost due to disease. Everyone around the victim suffers, emotionally and financially. Of course, other conditions partner cancer – mental illness, digestive tract impairment, metabolic dysregulation.
Wellbeing narratives that fail to look at environmental and dietary cancer drivers are, excuse me, bullshit.
Without addressing real food and the relationship with cancer, all the equity/inequity rhetoric in the world fails. It’s political greenwashing.
Why do I care? I watched my stepmother die of cancer painfully and slowly when I was 23, and then my father die of cancer quickly and traumatically when I was 27. Trips to Melbourne as a teenager inevitably involved a round trip for my step-mother for cancer treatment to the Peter McCallum cancer centre. Neither of them changed their diets markedly and both of them followed medical protocols. A 50-year-old cousin died from glioblastoma, leaving a wife and two young children. So yes, like many, if not most, cancer is ‘a thing’ for me.
Cancer incidence is increasing.
The war on cancer seems to – eternally - leave environmental causes outside.
A burgeoning literature is indicating that there are strong associations between diet and the aetiology of cancer – this includes the top 4 cancers, colorectal, prostate, lung and breast. Vaping is new, but the food-grade ingredients may be part of why lung cancer should not only be connected to smoking. Our diets and our exposures have radically changed, from that of our grandparents.
Cancer and diet are a ‘thing’. The relationship of ultraprocessed foods and chronic illness is getting stronger and stronger. See here, here, here and here. It’s not just diet that we’re slow to look at, it’s environmental drivers in general.
Disturbed glucose metabolism in cancer patients has been understood for over 50 years. It seems that ultraprocessed foods impair mitochondrial activity; and harm the microbiome (and scientists are learning about microbiome and cancer associations constantly).
And this 2002 paper on Cancer and Inflammation has been cited 17,000 times.
Scientific literature has been slow to explore the association of processed foods in the diet and cancer. Our ancestors were exposed to less dietary synthetic chemicals (formulation additives and pesticide sprays); more whole food fibre, and complex mixtures of fibre and more protein. Protein came from natural fats – from dairy, crops and meat. Food was seasonal.
Yes, there is also the question of ‘bad luck’. Since mutations occur at a low rate during cell division, there will be a proportion of cancers that are just a consequence of natural cell division.
Don’t let the ‘bad luck’ narrative scare you into thinking cancer is inevitable. Heritability and occupational risk factors are just part of the picture. For most of - cancer risk is increasing every decade. That isn’t our genes - that’s our environment. Cancer diagnoses are occurring at younger and younger ages:
Since 1990, the incidence and deaths of early onset cancers have substantially increased globally. Early onset breast, tracheal, bronchus and lung, stomach and colorectal cancers showed the highest mortality and burden in 2019.

Nutrient deficiencies and environmental insults (which can be driven by low nutrient processed-food diets that promote internal inflammation) - change gene function epigenetically.
Without certain nutrient cofactors, our metabolic health simply can’t be sustained, add toxicity which drives inflammation, and your body is fighting a losing battle.
Yes, you can drive disease, but which way do you want to drive it?
Why is diet a trite afterthought in New Zealand’s 2019-2029 cancer policy?
NZ GOVERNMENT INFO & GUIDELINES FOR FOOD & DIET
Recent reports on New Zealand dietary habits do not discuss the extent of ultraprocessed food in the diet. In 2022 reports on the dietary habits of adults and children – the only ‘processed’ item was processed meat. Sweet baked things and takeaways were discussed, but not other processed goods such as chips, noodles. The quantity of bread and cereal-based products as a proportion of diet in children or adults was apparently explored but not reported. The frequency of consumption of red meat was reported (guidelines recommend three times a week with the fat chopped off). The health status of processed imitation meats was not discussed.
The 2020 adult guidelines recommend low-fat or unsaturated fat diets. Children should eat low fat diets (2015, 2023). Boys and girls under 12 require 4-5 servings of cereal, 1.5-3.5 servings of dairy, and 1-2.5 servings of protein per day (2023).
Government guidelines are looking more and more contradictory when they tell us - for example, that grass-fed meat and butter are scary (but fail to balance the nutrient gain) but grainy toast (with pesticide contamination) is perfectly fine.
POLICY FOR CANCER?
The Labour and National Ministers of Health, and Ministers for Business, Innovation and Employment, keep cancer and the relationship of cancer with diets, well outside policy. They do it three ways: 1. they don’t construct policy that declares diets are a critical driver of cancer risk; 2. they don’t finance long-term research on this relationship; and 3. they don’t finance information distribution at scale to inform and educate the public on the scientific basis for the relationship.
New Zealand’s 68-page Cancer Action Plan 2019–2029 discusses the need for people to make healthy choices, but only mentions ‘nutrition’ twice. One page discusses the need to establish healthy or supportive food environments. But that’s about all.
Outcome 3: Investment in the prevention of cancer will ultimately make the largest contribution to reducing the burden of cancer in New Zealand and to achieving equity in outcomes.
But there’s no funding. Structure and function – no policy for funding results in no funding.
WHAT DO GOVERNMENT $$$ BUDGETS REVEAL?
The Ministry of Health’s 2023/24 budget discusses cancer in relation to diagnosis, but doesn’t allocate money to supporting food, nutrition or diet.
Pharmac’s primary statutory objective is ‘to secure for eligible people in need of pharmaceuticals.’ With this in mind, all the discussion about health in this graph might be able to be substituted with ‘medical’.
Pharmac funds New Zealand’s $1.186 billion medicines budget, and has funded 52 different cancer medications in the past ten years, and two new immunotherapy treatments for lung cancer have been approved. Pharmac does fund some nutritional therapies, but these are primarily outside scope. Therefore Pharmac won’t proactively undertake reviews to identify the if nutritional therapies make a difference to health outcomes. This is why the annual reviews don’t tend to discuss nutritional therapies and equity discourse concerns access to pharmaceutical drugs.
Perhaps we need to understand what health benefits really mean, when diet isn’t factored into health across whole of government.
WHAT DOES OUR SCIENCE SYSTEM SAY?
When we’re attempting to heal from a complex chronic condition (including mental illness) many doctors will suggest that there is not much evidence for a particular modality. The problem is, they went to medical school. They didn’t have nutrition education beyond a couple of weeks, and there are no established systems funnelling of recently published data on nutrition into your local medical centre.
There’s no place in New Zealand that is responsible - at a distance from the political Ministries - for looking at and reviewing scientific data on health and nutrition.
Funding for science research is controlled by MBIE and is in the ‘economic development’ section of budget appropriations (rather than science or education). The Vote Business, Science and Innovation 2023/2024 total budget is $3,735.3 million – of which $1,475 million is for scientific research. Of this, there is no dedicated food and nutrition research that is clearly delineated. $10.6 million is allocated for ‘high value nutrition’ - but that’s marked for public-private collaborations, primarily concerned with value adding to increase export market opportunities for premium NZ food products (a good endeavour).
The ‘Healthier Lives’ National Science Challenge (NSC) doesn’t have a scope that would encourage researchers to consider the relationship between ultraprocessed food and cancer. So if researchers can’t get the funding, studies will be fewer, they will be short term, they will have smaller study populations… we are the poorer for it.
Universities have nutrition departments, but they are dependent on funding through entities such as the NSC and Health Research Council. So long term funding for Uni’s is uncertain and ad hoc. A scientist might do research in one area, but be reluctant to generalise on a ‘political issue’ (which is what happens when you discuss diet and cancer) and seen by university management as taking a ‘political’ position.
It seems that a scientist will be seen as ‘political’ if they discuss food and nutrition as treatment for a chronic disease, but not if they discuss a new biologic drug.
Scientific research for nutrition and diet is minor and ad hoc in comparison to the overall science research budget. MBIE and the Ministry of Health’s Health Research Strategy 2017-2027 steers science and research away from complex interdisciplinary research to identify the drivers of disease. Believe me, I know.
Current policy binds funding committees so that complex proposals get pushed down for funding because outside the box thinking can’t be identified as ‘excellent’. The Health Research Council is correct, health research saves lives. But the MoH and MBIE’s policy bind, helps us understand why it’s easy for funding to tentatively fund small trials on nutrition and diet but why there’s so few really big trials over years. Less scientists willing to be the public face of complex disease, because they’re more easily funded to do applied research rather than basic science.
WHAT DO OUR MEDICAL DOCTORS SAY?
Doctors receive payments when they screen patients for certain diseases and when they prescribe certain drugs. But doctors do not receive incentive payments to reverse disease (which might reduce drug intakes and positively impact Pharmac’s budget).
Questions for your medical doctor or GP:
How many years of education and much nutrition and dietary education did they receive?
Where do they go to gather nutritional and dietary advice for patients?
Are they comfortable making recommendations that differ from the Ministry of Health?
Have they talked to the New Zealand Medical Council about their capacity to give nutritional and dietary advice?
If your doctor has gone on to undertake extensive research in diet and nutrition, are they encouraged to discuss nutrition and diet based on their expertise by their professional associations?
It’s likely doctors’ responses will be quite cautious and guarded, that any nutritional advice will align with the Ministry of Health’s position.
WHAT DRIVES CANCER?
Genes - 5-10%. - it’s been known for about 50 years that most cancers are environmentally driven. Parsa (2012):
Up to 93% of all human cancers are non-hereditary which is caused by interaction with environmental factors. Only 7% of all human cancers are hereditary.
Inflammation. Metabolic syndrome and diabetes. Loneliness. Lower nutritional biomarker scores. Professions where you are exposed to toxicants and heavy metals. Ultraprocessed foods. Persistent stress. Genes play a relatively small role in the aetiology of cancer.
But these complex drivers are outside policy rubrics which set people on a diagnosis and treatment round-a-bout. But they’re important to understand, because survivors are survivors at 1-5 years, and cancer comes back. Every doctor and oncologist understand that cancer recurrence is a massively downplayed issue.
We can see from government policy that the saturated fat and animal protein consumption is de-emphasised, while relatively large quantities of cereals are encouraged. Government policy shows us there are little funding pathways for non-medical nutritional therapies, and that science policy makes little room for looking at dietary drivers of cancer (and other illnesses).
With this in mind we can see why the Ministry of Health doesn’t discuss what a ketogenic diet might achieve for people with chronic illness? Why New Zealand is yet to have research approved to understand the role of ketogenic diets and the reversal of disease? This sort of research is not in scope. There are pockets of very determined researchers out there, but their research is piecemeal and certainly not financed through the main health research funding pathway.
Ketogenic diets which increase the protein and fat content in the diet are pervasively inconsistent with policy guidelines. Never mind that insulin resistance is directly associated with diabetes and cardiovascular health.
I’m not saying that keto is the whole truth and nothing but the truth – it’s just that research and policy looking at the relationship of health with ultraprocessed food consumption, and that emphasise the foods our ancestors ate – including fat and meat protein – are outside funding scopes (‘research themes’).
Our impressive medical budget - $1.186 billion – for medicine mainly targeted to managing (not healing) chronic disease, dwarfs nutrition funding, which is, basically, not ‘a thing’.
The $Billion$ medical budget belies the insane policy gap that puts ultraprocessed food, and answers to the processed food epidemic, including research on ketogenic diets, largely outside consideration. The best effort I can find is a 2021 grant of $1.4 million for a 3 year study. This science is drip-fed.
How can the MoH or Ministers responsible for protecting health carry out their duties with such barriers to research, to informed policy and for doctors moving to a system where they are compensated for promoting health?
Why have shadow ministers for the health portfolio persistently ignored these glaring contradictions?
Does it make sense that more and more people are distrusting the ‘medical system’ and a machinery of government whose policy seems to reflect international rubrics - that government guidelines reflect a level of predetermination that then becomes locked into policy…
… while obviously failing to address nuance, and failing to keep updated on the latest literature?
It’s unethical. But big food and big pharma love it.
What a game.
On a personal note, my Dad developed rapid-onset dementia (it happened right after his booster, sigh). A strict keto diet (we are doing the Bredeson protocol) has been instrumental in halting the decline. Our GP is very supportive. It's worth looking into if you have a loved one with dementia.
Regarding the conflicts which make it impossible for the Ministry of Health to promote actual health, I first learned of this some years ago when I became curious about our problem with childhood obesity. In summary - McDonalds is in charge of looking after our children's health. My notes from the MOH documentation won't fit in a comment box, so I am pasting them as a google doc in case you are interested in see them. I'm sure they will all be very familiar to you! Thanks for another amazing article, Jodi.
https://docs.google.com/document/d/1Qo2lw6ZXui-UwKmt3OXq_oQ_ChhOxWFmkstYGljOkz0/edit?usp=sharing
N=1 Carnivore WOE here, I'm reversing every ill from years of following a standard diet, nutritional guidelines and the processed food addictions one steak at a time. I've never felt better, my doctor can't quite fathom my improved bloodwork, I keep saying it's ketones. I was diagnosed with a rare cancer, thanks to the surgeon and going carnivorous I've remained in remission. I do enjoy reading your work. Thanks.